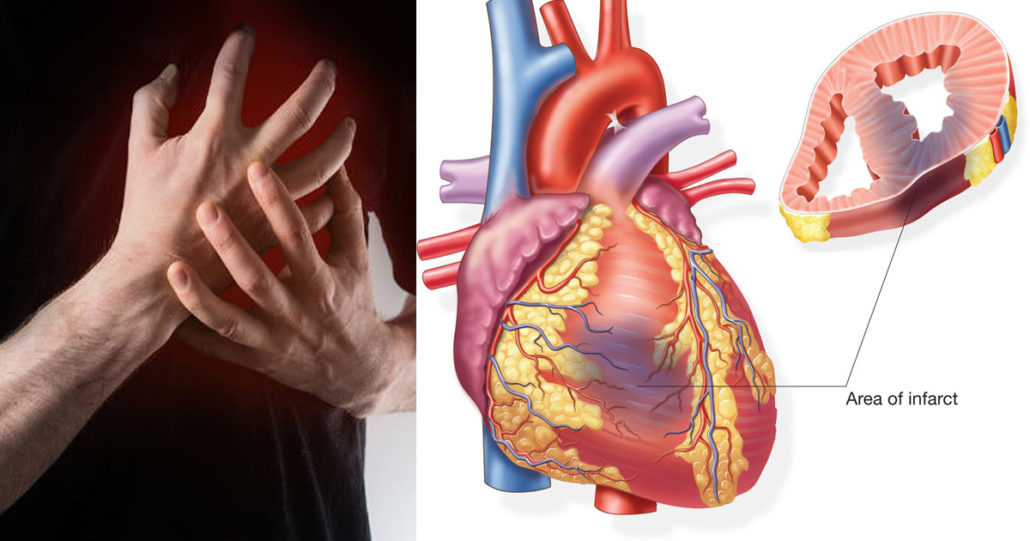
Myocardial Infarction (Heart Attack)
Myocardial infarction (MI) (i.e., heart attack) is the irreversible death (necrosis) of heart muscle secondary to prolonged lack of blood flow and oxygen to the heart muscle (ischemia). Approximately 1.5 million cases of MI occur annually in the United States.
History
The patient’s history is critical in diagnosing myocardial infarction and sometimes may provide the only clues that lead to the diagnosis in the initial phases of the patient presentation.
Patients with typical acute MI usually present with chest pain and may have prodromal symptoms of fatigue, chest discomfort, or malaise in the days preceding the event; alternatively, typical ST-elevation MI (STEMI) may occur suddenly without warning.
The typical chest pain of acute MI is intense and unremitting for 30-60 minutes. It is retrosternal and often radiates up to the neck, shoulder, and jaws, and down to the left arm. The chest pain is usually described as a substernal pressure sensation that is also perceived as squeezing, aching, burning, or even sharp. In some patients, the symptom is epigastric, with a feeling of indigestion or of fullness and gas.
The patient may recall only an episode of indigestion as an indication of myocardial infarction. In some cases, patients do not recognize chest pain, possibly because they have a stoic outlook, have an unusually high pain threshold, have a disorder that impairs function of the nervous system and that results in a defective anginal warning system (e.g., diabetes mellitus), or have obtundation caused by medication or impaired cerebral perfusion. Elderly patients with preexisting altered mental status or dementia may have no recollection of recent symptoms and may have no complaints whatsoever.
MI occurs most often in the early morning hours. Mechanisms that may explain this circadian variation include the morning increase in sympathetic tone leading to increases in blood pressure, heart rate, coronary vascular tone, and myocardial contractility; the morning increase in blood viscosity, coagulability, and platelet aggregability; and the increased morning levels of serum cortisol and plasma catecholamines leading to sympathetic overactivity, thereby resulting in increased myocardial demand.
Initial rapid evaluation should include a brief history and a focused physical examination. Important elements of the history, such as characteristics of the pain and associated symptoms, and risk factors for cardiovascular disease, are used to determine the likelihood of acute coronary syndrome (ACS) and to predict clinical outcomes.
A high index of suspicion for MI is required, especially when evaluating women, patients with diabetes, older patients, patients with dementia, patients with a history of heart failure, cocaine users, patients with hypercholesterolemia, and patients with a positive family history for early coronary disease. Positive family history includes any first-degree male relative aged 45 years or younger or any first-degree female relative aged 55 years or younger who experienced an MI or the need for coronary revascularization.
Other symptoms of myocardial infarction include the following:
- Anxiety, commonly described as a sense of impending doom
- Pain or discomfort in areas of the body, including the arms, left shoulder, back, neck, jaw, or stomach
- Lightheadedness, with or without syncope
- Cough
- Nausea, with or without vomiting
- Profuse sweating
- Shortness of breath
- Wheezing
- Rapid or irregular heart rate
- Fullness, indigestion, or choking feeling
Physical Examination
Physical examination findings for myocardial infarction (MI) can vary; one patient may be comfortable in bed, with normal examination results, whereas another patient may be in severe pain, with significant respiratory distress and a need for ventilatory support.
Patients with ongoing symptoms usually lie quietly in bed and appear pale and diaphoretic.
Vital signs
Heart rate
The patient’s heart rate is often increased (tachycardia secondary to sympathoadrenal discharge). The pulse may be irregular because of ventricular ectopy, an accelerated idioventricular rhythm, ventricular tachycardia, atrial fibrillation or flutter, or other supraventricular arrhythmias.
Depressed heart rate may also be present in some cases. Bradyarrhythmias may be attributable to impaired function of the sinus node. An atrioventricular (AV) nodal block or infranodal block may also be present.
Unequal palpable pulses can be suggestive of the presence of aortic dissection, which commonly presents with chest pain radiating to the back, accompanied by a blood pressure difference of 15 mm Hg or greater between both arms and an aortic regurgitation murmur.
Blood pressure
In general, the patient’s blood pressure is initially elevated (hypertension because of peripheral arterial vasoconstriction resulting from an adrenergic response to pain, anxiety, and ventricular dysfunction). However, it is not uncommon to have increased blood pressure as the precipitant of acute MI.
Alternatively, hypotension can also be seen. Usually, this indicates either right ventricular MI or severe left ventricular dysfunction due to a large infarct area or impaired global cardiac contractility.
Respiratory rate
The respiratory rate may be increased in response to pulmonary congestion or anxiety.
Temperature
Fever is usually present within 24-48 hours, with the temperature curve generally parallel to the time course of elevations of creatine kinase (CK) levels in the blood. Body temperature may occasionally exceed 102°F.
Neck veins
In patients with acute inferior-wall MI with right ventricular involvement, distention of neck veins is commonly described as a sign of failure of the right ventricle. The impaired right ventricular function also leads to systemic venous hypertension, edema, and hepatomegaly.
Heart
On palpation, lateral displacement of the apical impulse, dyskinesis, a palpable S4 gallop, and a soft S1 sound may be found. These signs indicate diminished contractility of the compromised left ventricle.
Paradoxical splitting of S2 may reflect the presence of left bundle-branch block or prolongation of the pre-ejection period with delayed closure of the aortic valve, despite decreased stroke volume.
A new mitral regurgitation murmur (typically holosystolic near the apex) indicates papillary muscle dysfunction or rupture, or mitral annular dilatation; it may be audible even when cardiac output is substantially decreased.
A holosystolic murmur that radiates to the midsternal border and not to the back, possibly with a palpable thrill, suggests a ventricular septal rupture; such a rupture may occur as a complication in some patients with full-thickness MIs. With resistive flow and an enlarged pressure difference, the ventricular septal defect murmur becomes harsher, louder, and higher in pitch than before.
A pericardial friction rub may be audible as a to-and-fro rasping sound; it is produced through sliding contact of inflammation-roughened surfaces.
Chest
Rales or wheezes may be auscultated; these occur secondary to pulmonary venous hypertension, which is associated with extensive acute left ventricular MI. Unilateral or bilateral pleural effusions may produce egophony at the lung bases.
Abdomen
Patients frequently develop tricuspid incompetence; hepatojugular reflux may be elicited even when hepatomegaly is not marked.
A pulsatile abdominal mass may suggest an abdominal aortic aneurysm.
Extremities
Peripheral cyanosis, edema, pallor, diminished pulse volume, delayed rise, and delayed capillary refill may indicate vasoconstriction, diminished cardiac output, and right ventricular dysfunction or failure. Pulse and neck-vein patterns may reveal other associated abnormalities, as previously discussed.
Myocardial Infarction Workup
The objectives of laboratory testing and imaging include the following:
- To determine the presence or absence of myocardial infarction (MI) for diagnosis and differential diagnosis (point-of-care testing and testing in central laboratory of cardiac troponin levels)
- To characterize the locus, nature (ST-elevation MI [STEMI] or non–ST-elevation MI [NSTEMI]), and extent of MI (ie, to estimate infarct size)
- To detect recurrent ischemia or MI (extension of MI)
- To detect early and late complications of MI
- To estimate the patient’s prognosis
The electrocardiogram (ECG) is the most important tool in the initial evaluation and triage of patients in whom an acute coronary syndrome (ACS) is suspected.
Laboratory tests used in the diagnosis of myocardial infarction (MI) include the following:
- Cardiac biomarkers/enzymes: The American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology (ESC) guidelines recommend cardiac troponin as the only cardiac biomarker that should be measured at presentation in patients with suspected MI, due to its superior sensitivity and accuracy. Troponin is a contractile protein that is not normally found in serum; it is released only when myocardial necrosis occurs.
- Complete blood cell (CBC) count
- Comprehensive metabolic panel
- Lipid profile
Electrocardiography
- The electrocardiogram (ECG) is the most important tool in the initial evaluation and triage of patients in whom an acute coronary syndrome (ACS) is suspected. Obtaining an ECG by emergency medical services (EMS) personnel at the site of first medical contact in patients with symptoms consistent with ST-elevation myocardial infarction (STEMI) not only confirms the diagnosis in more than 80% of cases, but also helps to detect life-threatening arrhythmias and allows early and prompt defibrillation therapy, if indicated.
- Expert medical societies and organizations including the American College of Cardiology (ACC), the American Heart Association (AHA), and the European Society of Cardiology (ESC) have emphasized the importance of obtaining a 12-lead ECG in a timely fashion (≤10 mins of presentation) in their recommendations for management of ACS and STEMI, with interpretation by an experienced physician.
ECGs should be performed serially upon presentation to evaluate progression and assess changes with and without pain. An ECG is a rapid, low-risk, relatively low-cost measure.
Because the symptoms of acute MI can be subtle, an ECG should be performed on any patient who is older than age 45 years and is experiencing any form of thoracoabdominal discomfort, including new epigastric pain or nausea.
In younger patients, an ECG should be considered when suggestive symptoms are present or when risk factors exist for early coronary artery disease. Younger patients are disproportionately represented in missed cases.
Different ECG abnormalities
ECG is an effective tool to distinguish between acute MI and the myocardial ischemia that usually precedes it, as not all patients with myocardial ischemia will develop MI.
Transitioning from ischemia to infarction results in precise sequential electrical abnormalities captured on ECG. Moreover, these changes are localized, which helps in detection of the involved region of the myocardium in most cases.
In STEMI, typical ST-segment elevation persists for hours and is followed by inversion of T waves during the first few days and by the development of Q waves. However, initial ST depression or T-wave inversion associated with MI is difficult to differentiate from that seen in the presence of ischemia without MI or other unrelated conditions. ST-segment depression followed by T-wave inversion without the evolution of Q waves may result from non–ST-elevation MI (NSTEMI) or from subendocardial ischemia without MI.
High-probability ECG features of MI are the following:
- ST-segment elevation greater than 1 mm in two anatomically contiguous leads
- The presence of new Q waves
Intermediate-probability ECG features of MI are the following:
- ST-segment depression
- T-wave inversion
- Other nonspecific ST-T wave abnormalities
Low-probability ECG features of MI are normal ECG findings. However, normal or nonspecific findings on ECGs do not exclude the possibility of MI.
Special attention should be made if there is diffuse ST depression in the precordial and extremity leads associated with more than 1 mm ST elevation in lead aVR, as this may indicate stenosis of the left main coronary artery or the proximal section of the left anterior descending coronary artery.
Localization of the involved myocardium based on distribution of ECG abnormalities in MI is as follows:
- Inferior wall – II, III, aVF
- Lateral wall – I, aVL, V4 through V6
- Anteroseptal – V1 through V3
- Anterolateral – V1 through V6
- Right ventricular – RV4, RV5
- Posterior wall – R/S ratio greater than 1 in V1 and V2, and T-wave changes in V1, V8, and V9
True posterior-wall MIs may cause precordial ST depressions, inverted and hyperacute T waves, or both. ST-segment elevation and upright hyperacute T waves may be evident with the use of right-sided chest leads.
Hyperacute (symmetrical and, often, but not necessarily pointed) T waves are frequently an early sign of MI at any locus.
The appearance of abnormalities in many ECG leads often indicates extensive injury or concomitant pericarditis.
The characteristic ECG changes may be seen in conditions other than acute MI. For example, patients with previous MI and left ventricular aneurysm may have persistent ST elevations resulting from dyskinetic wall motion, rather than from acute myocardial injury. ST-segment changes may also be the result of misplaced precordial leads, early repolarization abnormalities, hypothermia (elevated J point or Osborne waves), or hypothyroidism.
False Q waves may be seen in septal leads in hypertrophic cardiomyopathy (HCM). They may also result from cardiac rotation.
Substantial T-wave inversion may be seen in left ventricular hypertrophy with secondary repolarization changes.
The QT segment may be prolonged because of ischemia or electrolyte disturbances.
Saddleback ST-segment elevation (Brugada epsilon waves) may be seen in leads V1-V3 in patients with a congenital predisposition to life-threatening arrhythmias. This elevation may be confused with that observed in acute anterior MI.
Diffuse brain injuries and hemorrhagic stroke may also trigger changes in T waves, which are usually widespread and global, involving all leads.
Convex ST-segment elevation with upright or inverted T waves is generally indicative of MI in the appropriate clinical setting. ST depression and T-wave changes may also indicate evolution of NSTEMI.
Patients with a permanent pacemaker may confound recognition of STEMI by 12-lead ECG due to the presence of paced ventricular contractions.
To summarize, non-ischemic causes of ST-segment elevation include left ventricular hypertrophy, pericarditis, ventricular-paced rhythms, hypothermia, hyperkalemia and other electrolyte imbalances, and left ventricular aneurysm.
Cardiac Biomarkers
In the past, different cardiac biomarkers have been used to evaluate patients with suspected acute myocardial infarction (MI) (acute coronary syndrome [ACS] and ST-elevation MI [STEMI]). The cardiac-specific troponins I and T, creatine kinase (CK), the MB isoenzyme of creatine kinase (CK-MB), and myoglobin have been used as surrogates for myocardial necrosis.
Cardiac troponin detection and quantification has improved dramatically over the years as advanced technology allows obtaining cardiac troponin assays running on automated platforms with a high degree of sensitivity. Although implementation of point-of-care testing (POCT) for cardiac biomarkers may seem to improve early diagnosis, with an advantage of having a shorter turnaround time, this comes at the expense of substantial lower sensitivity and accuracy compared to results obtained from central laboratory testing.
Serial measurement of cardiac troponins after the initial level is obtained at presentation, 3 to 6 hours after symptom onset, is recommended. If initial levels are negative, additional measurements beyond the 6-hour mark should be obtained.
The graph below demonstrates the timing of release of various cardiac biomarker peaks after the onset of MI.
Timing of release of various cardiac biomarker peaks after the onset of myocardial infarction
Cardiac Troponin
Troponin is a contractile protein that normally is not found in serum. It is released only when myocardial necrosis occurs. Of the three troponin subunits, two (troponin I and troponin T) are derived from the myocardium.
Highly sensitive assays can now detect cardiac troponin in patients with acute myocardial infarction (MI) with a high degree of certainty. This has led to the change in clinical practice guidelines to recommend relying solely on the results of sensitive or high-sensitive troponin I or troponin T assays for diagnostic and prognostication purposes in patients with symptoms suggestive of acute MI.
Serum levels increase within 3-12 hours from the onset of chest pain, peak at 24-48 hours, and return to baseline over 5-14 days.
Measurement of troponin levels for patients with chest pain in the emergency setting has been studied extensively. Baseline measurement of troponin levels followed by serial measurements of troponin 3 hours afterward should be performed; both the absolute value of the troponin level as well as the degree of change in the troponin level should be considered. This has been associated with better performance in an accurate diagnosis of acute MI.
B-Type Natriuretic Peptide
B-type natriuretic peptide (BNP) is a 32-amino acid polypeptide secreted by the ventricles of the heart in response to excessive stretching of cardiomyocytes.
Measurement of BNP or N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) for the diagnosis of acute myocardial infarction (MI) is not recommended for diagnosis of MI, but these biomarkers have utility in risk stratification and prognostication of patients with acute MI who may have congestive heart failure.
Other Laboratory Studies
Complete blood cell count
Obtain a complete blood cell (CBC) count if myocardial infarction (MI) is suspected in order to rule out anemia as a cause of decreased oxygen supply and prior to giving thrombolytic agents. Leukocytosis is also common, but not universal, in the setting of acute myocardial infarction.
A platelet count is necessary if IIb/IIIa agent is considered; furthermore, the patient’s white blood cell (WBC) count may be modestly elevated in the setting of MI, signifying an acute inflammatory state. The platelet count may become dangerously low after the use of heparin because of heparin-induced thrombocytopenia (HIT). The leukocyte count may be normal initially, but it generally increases within 2 hours and peaks in 2-4 days, with predominance of polymorphonuclear leukocytes and a shift to the left. Elevations generally persist for 1-2 weeks.
Chemistry profile (comprehensive metabolic panel)
In the setting of MI, closely monitor potassium and magnesium levels. The creatinine level is also needed, prior to cardiac catheterization and prior to initiating treatment with an angiotensin-converting enzyme (ACE) inhibitor. Blood glucose levels are important to measure, as many patients are first diagnosed with diabetes when they present with MI.
Although not routinely measured, the erythrocyte sedimentation rate (ESR) rises above reference range values within 3 days and may remain elevated for weeks.
The serum lactate dehydrogenase (LDH) level rises above the reference range within 24 hours of MI, reaches a peak within 3-6 days, and returns to the baseline within 8-12 days.
Blood oxygenation should be checked and repeatedly corrected if any clinical findings suggest hypoxemia; hypoxemia may result from pulmonary congestion, atelectasis, or ventilatory impairment secondary to complications of MI or excessive sedation or analgesia. Fingertip oximetry may be adequate in the absence of carbon dioxide retention and may obviate puncture to assess arterial blood gases (ABGs). Such puncturing may lead to bleeding in patients being treated with thrombolytic drugs. However, normal oxygen saturation does not exclude impending respiratory failure.
Lipid profile
A lipid profile may be helpful if obtained upon presentation, because levels can change after 12-24 hours of an acute illness. However, regardless of the lipid profile results, initiation of a high-intensity statin is recommended in all patients with acute coronary syndrome.
Cardiac Imaging
The role of imaging in the work-up of acute myocardial infarction (MI) is broad, but the procedures are primarily used to confirm or rule out coronary artery disease (CAD). Furthermore, imaging may help to define the anatomy and degree of myocardial perfusion abnormalities. In lower-risk individuals in whom acute coronary syndrome (ACS) is suspected and who do not have serial electrocardiographic (ECG) changes or positive serial cardiac biomarker findings, some form of stress testing may help to confirm the diagnosis and guide therapy.
For individuals with highly probable or confirmed ACS, consult with a cardiologist so that urgent coronary angiography can be performed; this procedure can be used to definitively diagnose or rule out CAD. Based on the angiographic result and patient comorbidities, subsequent treatment recommendations can be made, which may include medical therapy, percutaneous coronary intervention (PCI), or coronary artery bypass graft (CABG) surgery.
Multidetector computed tomography (MDCT) coronary angiography may be considered as an alternative to invasive angiography to exclude ACS when there is a low to intermediate likelihood of CAD and when cardiac troponin and/or ECG results are inconclusive. This imaging modality can be used in the emergency department for triage of patients with chest pain.
The use of myocardial perfusion imaging (MPI) with single-photon emission CT (SPECT) or positron emission tomography (PET) scanning in the emergency department for low-risk patients has a low yield for detecting ischemia. Therefore, use of SPECT or PET scanning to diagnose MI in patients with negative serial troponin results and nondiagnostic ECGs is not routinely performed.
Echocardiography is highly recommended and is required to evaluate ventricular function and wall-motion abnormalities. It is also used to identify pericardial effusion, ischemic mitral regurgitation, and cardiac tamponade that may complicate acute MI.
Management
The first goal for healthcare professionals in management of acute myocardial infarction (MI) is to diagnose the condition in a very rapid manner.
Initial therapy for acute MI is directed toward restoration of perfusion as soon as possible to salvage as much of the jeopardized myocardium as possible. This may be accomplished through medical or mechanical means, such as percutaneous coronary intervention (PCI), or coronary artery bypass graft (CABG) surgery.
Although the initial treatment of the different types of acute coronary syndrome (ACS) may appear to be similar, it is very important to distinguish whether the patient is having an ST-elevation MI (STEMI) or a non–STEMI (NSTEMI), because definitive therapies differ between these two types of MI. Particular considerations and differences involve the urgency of therapy and the degree of evidence regarding different pharmacologic options.
Over the last decade, inhibition of proprotein convertase subtilisin/kexin type 9 (PCSK9) has emerged as a promising target to reduce residual cardiovascular disease risk. PCSK9 is a protein that binds to low-density lipoprotein (LDL) receptors (LDLR) to promote their degradation. Monoclonal antibodies inhibit PCSK9 and thus prevent LDLR degradation. This action will increase the number of LDLRs and subsequently increase the clearance of LDL, ultimately lowering LDL-C levels.
In December 2017, the FDA approved the first PCSK9 inhibitor, evolocumab (Repatha), for the prevention of strokes, heart attacks, and coronary revascularizations.The approval was based on data from the evolocumab cardiovascular outcomes study (FOURIER). In the FOURIER clinical trial, evolocumab demonstrated significant benefits for 27,564 patients with established cardiovascular disease. The study revealed that when used in addition to optimized statin therapy, evolocumab reduced the risk of heart attack by 27%, the risk of stroke by 21%, and the risk of coronary revascularization by 22%. In addition, evolocumab showed a statistically significant 15% reduction in the risk of the primary composite endpoint, which included hospitalization for unstable angina, coronary revascularization, heart attack, stroke, or cardiovascular death.
2017 American Heart Association/American College of Cardiology (AHA/ACC) clinical performance and quality measures for adults with STEMI and NSTEMI
Revised STEMI and NSTEMI measures
Statin use for patients with AMI (acute myocardial infarction)
Evaluation of LVEF (left ventricular ejection fraction)
P2Y12 receptor (clopidogrel, ticagrelor, prasugrel) inhibitor prescribed at discharge. All 3 medications are inhibitors of the P2Y12 receptor and are recommended in addition to aspirin (as part of a dual antiplatelet regimen) to reduce recurrent ischemic events after AMI.
New STEMI/NSTEMI measures
Immediate angiography for resuscitated out-of-hospital cardiac arrest in STEMI patients.
Noninvasive stress testing before discharge in conservatively treated patients to detect inducible ischemia in medically treated STEMI and NSTEMI patients.
Early cardiac troponin measurement (within 6 hours of arrival).
Participation in regional or national acute myocardial infarction registry to help track and assess the outcomes, complications, and quality of care for patients with AMI.
Risk score stratification for NSTEMI patients to dictate the appropriate strategy (invasive versus ischemic-guided) and the timing of the strategy (early versus late invasive) in patients with NSTEMI.
Early invasive strategy (within 24 hours) in high-risk NSTEMI patients.
Therapeutic hypothermia for comatose STEMI patients with out-of-hospital cardiac arrest.
Aldosterone antagonist at discharge.
Inappropriate in-hospital use of nonsteroidal anti-inflammatory drugs (NSAIDs) (caution against the use of these drugs after AMI).
Inappropriate prescription of prasugrel at discharge in patients with a history of prior stroke or transient ischemic attack (TIA) (caution against the use of prasugrel in patients with prior TIA/stroke, because of net clinical harm in these patients. The FDA also issued a black box warning on this.)
Inappropriate prescription of high-dose aspirin with ticagrelor at discharge (caution against the use of high-dose aspirin >100 mg among patients receiving ticagrelor. The FDA also issued a black box warning on this.)
Prehospital Care and Initial Management
Morbidity and mortality from MI are significantly reduced if patients and bystanders recognize symptoms early, activate the emergency medical service (EMS) system, and thereby shorten the time to definitive treatment. Trained prehospital personnel can provide life-saving interventions if the patient develops cardiac arrest. The key to improved survival is the availability of early defibrillation. Approximately 1 in every 300 patients with chest pain transported to the emergency department by private vehicle goes into cardiac arrest en route. In the United States, several studies have confirmed that patients with STEMI usually do not call 911, and only about 40% of patients with a confirmed coronary event used EMS.
All patients being transported for chest pain should be managed as if the pain is ischemic in origin unless clear evidence to the contrary is established. If available, advanced cardiac life support (ACLS)–trained unit should transport patients with hemodynamic instability or respiratory difficulty.
Prehospital notification by emergency medical services (EMS) personnel should alert emergency department staff to the possibility ofa patient with myocardial infarction (MI). EMS personnel should receive online medical advice for a patient with high-risk features; this allows for the early and prompt delivery of medical treatment and, most importantly, facilitates the transportation of patients to facilities with the appropriate level of care.
Specific prehospital care includes the following:
- Intravenous access, supplemental oxygen if the oxygen saturation (SaO2) is less than 90%, pulse oximetry
- Immediate administration of non-enteric-coated chewable aspirin en route
- Nitroglycerin for active chest pain, given sublingually or by spray
- Telemetry and prehospital electrocardiography (ECG), if available
Most deaths caused by MI occur early and are attributable to primary ventricular fibrillation (VF). Therefore, initial objectives are immediate ECG monitoring; electric cardioversion in cases of VF; and rapid transfer of the patient to facilitate prompt coronary assessment.
Prehospital integration of ECG interpretation has been shown to decrease “door-to-balloon time,” allow paramedics to bypass non–percutaneous coronary intervention (PCI)–capable hospitals in favor of PCI-capable facilities, and to expedite care by allowing an emergency department physician to activate the catheterization laboratory before the patient’s arrival.
Additional objectives of prehospital care by paramedical and emergency personnel include adequate analgesia (generally achieved with morphine); pharmacologic reduction of excessive sympathoadrenal and vagal stimulation; treatment of hemodynamically significant or symptomatic ventricular arrhythmias (generally with amiodarone and lidocaine); and support of cardiac output, systemic blood pressure, and respiration.
Prehospital fibrinolytic therapy by the administration of tissue-type plasminogen activator (t-PA), aspirin, and heparin may be given to patients with bona fide MI by paramedics, as guided by electrocardiographic findings, within 90 minutes of the onset of symptoms. This treatment improves outcomes, as compared with thrombolysis begun after the patient arrives at the hospital. Prehospital fibrinolytic therapy is not used widely in the United States due to the lack of resources to train EMS personnel or the lack of funding for necessary equipment. However, it is more widespread in some regions in Europe and the United Kingdom.
Emergency Department Care and In-Hospital Management
Triage and evaluation
Because acute coronary syndrome (ACS) is a spectrum of conditions, initial evaluation to establish a working diagnosis is crucial, as this will dictate management owing to some differences in management steps and timelines for each component of the ACS spectrum.
All patients presenting to the emergency department with symptoms suggestive of acute myocardial infarction (MI) should be evaluated with a targeted history and focused physical examination. A 12-lead electrocardiogram (ECG) interpreted by an experienced physician should be completed within 10 minutes of arrival, in addition to establishing intravenous (IV) access.
Initial management
The initial management of the overall management plan for patients with acute MI has the following aims:
- Restoration of the balance between oxygen supply and demand to prevent further ischemia
- Pain relief
- Prevention and treatment of complications
Oxygen
Continuous oxygen saturation monitoring by pulse oximetry is needed for all patients.
Supplemental oxygen by a mask or nasal cannula is indicated only for patients who are breathless, hypoxic (oxygen saturation < 90% or PaO2< 60 mm Hg), or who present with heart failure. The use of oxygen in patients with acute MI who don’t fall into one of the three above-mentioned categories remains uncertain, with some studies suggesting possible harm in such patients.
Aspirin
All patients presenting with ACS should receive non-enteric-coated chewable aspirin in a dose of at least 162 to 325 mg, unless there is a clear history of aspirin allergy. Patients with aspirin intolerance still should receive aspirin at presentation.
Chewable aspirin is preferred, as this promotes rapid absorption into the bloodstream to achieve faster therapeutic levels.
Reduction of cardiac pain
Nitrates
Nitrates are potent vasodilators, and they act mainly to relax the venous system. Systemic venodilation results in reduction of venous blood return to the heart (i.e., reducing the ventricular preload); this will lead to reduction of the workload of the heart, less oxygen demand, and reduction in ischemic pain. Nitrates are also the most commonly used agents to reduce cardiac chest pain related to ischemia via coronary vasodilation; however, their use is not associated with reduction in ACS-associated mortality.
Nitrates are usually given as a 0.4 mg dose in a sublingual tablet, followed by close observation of the effect on chest pain and the hemodynamic response. If the initial dose is well tolerated, further nitrates can be administered. The most common side effect of nitrates are hypotension and headache.
When chest pain persists or recurs, IV nitrates are indicated, usually started at a dose of 5 to 10 µg/min and gradually increased until relief of chest pain is achieved.
Nitrates should not be used in patients presenting with marked hypotension or bradycardia, or if there is suspicion of right ventricular infarction.
Special attention should be made in taking the history of whether concomitant use of phosphodiesterase (PDE) inhibitors (e.g., sildenafil) has occurred within the last 24 to 72 hours, because this drug combination may lead to life-threatening hypotension.
Analgesia
Refractory or severe pain should be treated symptomatically with IV morphine.
The initial dose of morphine of 2 to 4 mg as an IV bolus can be given, with increments of 2 to 4 mg repeated every 5 to 10 minutes until the pain is relieved or intolerance is manifested by hypotension, vomiting, or depressed respiration. Should toxicity occur, a morphine antagonist such as naloxone is used for reversal. The patient’s blood pressure and pulse must be monitored; the systolic blood pressure must be maintained above 100 mm Hg and, optimally, below 140 mm Hg.
The use of other analgesic agents, such as nonsteroidal anti-inflammatory drugs (NSAIDs) should be avoided, if possible, as the use of these agents has been associated with adverse cardiovascular events.
ST-Elevation Myocardial Infarction
Management of ST-elevation myocardial infarction (MI) (STEMI) relies on two key components: rapid recognition and timely reperfusion. Therefore, systems must be implemented to prevent delay in management of patients who develop STEMI. Minimizing delays has been associated with improved overall outcomes as well as reduced mortality and long-term morbidity. Current clinical practice guidelines have emphasized adopting institutional quality improvement measures to reduce total ischemic time, which is the principal determinant of outcome; greatest emphasis is to be placed on the appropriate and timely use of some form of reperfusion therapy which is likely more important than the choice of therapy.
Some factors that may lead to shortening total ischemic time include the following:
- Prehospital electrocardiography (ECG) to diagnose STEMI to activate the percutaneous coronary intervention (PCI) team while the patient is en route to the hospital
- Emergency department physicians activate the PCI team
- A single call to a central page operator who activates the PCI team
- The goal is set for the PCI team to arrive in the catheterization laboratory within 20 minutes after being paged
- Timely data feedback and analysis are provided to members of the STEMI care team
Reperfusion
Early mechanical intervention (primary PCI) or pharmacologic reperfusion should be performed as soon as possible for patients with clinical presentation of STEMI within 12 hours of symptom onset and who have persistent ST-segment elevation or new or presumed new left bundle branch block (LBBB). In addition, it is reasonable to consider an early reperfusion strategy for patients presenting after more than 12 hours, provided there is clinical and/or ECG evidence of ongoing ischemia, with primary PCI being the preferred method in this population.
In the United States, only a minority of hospitals have the capability of performing primary PCI; therefore, a multifaceted community-wide approach that involves patient education, improvements in emergency medical services (EMS) and emergency department care, establishment of networks of STEMI-referral (non–PCI-capable) and STEMI-receiving (PCI-capable) hospitals, has been implemented to overcome this limitation.
For patients presenting to a PCI-capable hospital, emergent coronary angiography and primary PCI should be accomplished within 90 minutes. For patients presenting to a non–PCI-capable hospital, if they cannot be transferred to a PCI-capable hospital within 120 minutes, it is very important to rapidly assess the following to reach a decision about administration of fibrinolytic therapy:
- The time from onset of symptoms
- The risk of complications related to STEMI
- The risk of bleeding with fibrinolysis therapy
- The presence of shock or severe heart failure
- The time required for transfer to a PCI-capable hospital
Even when interhospital transfer times are short, there may be relative advantages to a strategy of immediate fibrinolytic therapy versus any delay to primary PCI for eligible patients who present within the first 1 to 2 hours after symptom onset.
Primary percutaneous intervention
PCI is defined as an emergent percutaneous coronary intervention in the setting of STEMI, without previous fibrinolytic treatment. It is the preferred reperfusion strategy in patients with STEMI, provided it can be performed expeditiously within clinical practice guidelines–mandated times and in high-volume centers with experienced interventional cardiology teams and skilled support staff.
PCI achieves superior reperfusion outcomes and is associated with less complications, death, and long-term complications of STEMI when compared to fibrinolytic therapy.
Current guidelines strongly recommend performing primary PCI in patients presenting with symptoms of less than 12 hours’ duration, or those who present with cardiogenic shock or who develop acute severe heart failure, irrespective of time of delay from onset of symptoms. Guidelines also recommend considering primary PCI for patients who present between 12 and 24 hours after onset of symptoms, provided there is ongoing clinical or ECG evidence of myocardial ischemia.
PCI of the non-infarct related artery (non-culprit artery) at the time of primary PCI of the culprit lesion is under active investigation. In a meta-analysis of 9 trials comprising 2991 patients with STEMI that compared complete multivessel PCI (revascularization of infarct-related and non-infarct-related arteries) to culprit-infarct-artery-only PCI, Vaidya et al. noted their findings suggested complete revascularization is safe in patients with STEMI and multivessel disease.Although complete vascularization appeared to be associated with lowered rates of major adverse cardiac events, cardiac death, and repeat revascularization in this population, no reduction in all-cause mortality and nonfatal MI was observed.
This method of reperfusion entails performing emergent coronary angiography, after establishing arterial access, which can be achieved via the radial or femoral artery. After identifying the anatomy of the coronary circulation and determining the culprit vessel, coronary stents are placed to establish reperfusion.
In patients with STEMI, the evaluation of 70% ST-segment resolution following primary PCI appears to be a 5-year independent predictor of patient-oriented composite endpoint, particularly all-cause death and any revascularization.The investigators suggested it may be used to identify those at high risk of very long-term cardiovascular events.
Drug-eluting stents (DES) or bare-metal stents (BMS) are used. However, if there are financial or social barriers that may limit patient compliance, an increased risk of bleeding, or an anticipated invasive or surgical procedure, the use of DES is not recommended.
Placement of coronary stents requires dual antiplatelet therapy for an extended time period (see the subsection “Antiplatelet agents,” below). The duration of therapy is dependent of the type of stent used.
Cardiac rupture is a major lethal complication of primary PCI for treatment of patients with STEMI. In a study comprising 1663 STEMI patients who underwent PCI of whom 33 (1.98%) developed cardiac rupture, investigators noted that the SYNTAX (Synergy between percutaneous coronary intervention with Taxus and Cardiac Surgery) Score II (SSII), which is used to assess anatomic and clinical risk in patients with stable coronary artery disease, is an independent predictor for cardiac rupture, which in itself has a poor prognosis. Increasing SSII tertiles were noted to be associated with a gradual rise in cardiac rupture occurrence.
Fibrinolysis
Fibrinolysis is an important reperfusion strategy, particularly in settings where primary PCI cannot be offered to STEMI patients within the recommended timelines. The benefit of fibrinolytic therapy in patients with STEMI is well established, with the largest benefit seen when administered early (within 12 hours after symptomatic onset) and in patients with the highest cardiovascular risk, including patients older than 75 years.
Fibrinolytic therapy may not be beneficial in patients who present more than 12 hours after symptom onset, although current practice guidelines recommend consideration of fibrinolysis in symptomatic patients with a large area of myocardium at risk (based on ECG or cardiovascular imaging) or hemodynamic instability if PCI is unavailable. See absolute and relative contraindications to fibrinolytic therapy in table 1, below.
Table 1. Absolute and Relative Contraindications to Fibrinolytic Therapy in Patients with STEMI
| Absolute Contraindications | Relative Contraindications |
|
|
Fibrinolytic therapy is associated with an excess of strokes, mainly due to cerebral hemorrhage, which is more commonly seen in patients with advanced age, lower weight, female sex, prior cerebrovascular disease, and hypertension on admission.
Different fibrinolytic agents are available, and table 2, below, lists different fibrinolytic agents with some of their key characteristics. In general, fibrin-specific agents are preferred when available.
Table 2. Fibrinolytic Agents Used in Management of STEMI.
| Fibrinolytic Agent | Dose | Fibrin Specificity | Antigenic | Patency Rate |
| Non-fibrin specific | ||||
| Streptokinase (no longer marketed in the US) | 1.5 million units IV given over 30–60 min | No | Yes | 60%–68% |
| Fibrin specific | ||||
| Tenecteplase
(TNK-tPA) |
30 mg for weight < 60 kg
35 mg for 60–69 kg 40 mg for 70–79 kg 45 mg for 80–89 kg 50 mg for >90 kg |
++++ | No | 85% |
| Reteplase (rPA) | 10-U IV boluses given 30 min apart | ++ | No | 84% |
| Alteplase (tPA) | Bolus 15 mg followed by infusion 0.75 mg/kg for 30 min (maximum 50 mg), then 0.5 mg/kg (maximum 35 mg) over the next 60 min; total dose not to exceed 100 mg. | ++ | No | 73%-84% |
| IV = intravenous; rPA = recombinant human tissue plasminogen activator; STEMI = ST-elevation myocardial infarction; tPA = tissue plasminogen activator; US = United States of America. | ||||
Coronary artery bypass grafting (CABG)
Despite great improvement of intraoperative myocardial preservation, CABG has a limited role in the acute management of STEMI. However, CABG remains indicated for cardiogenic shock, failed PCI, high-risk anatomy, surgical repair of a mechanical complication of STEMI (eg, ventricular septal rupture, free-wall rupture, or severe mitral regurgitation from papillary muscle dysfunction or rupture). CABG is also the preferred revascularization strategy for patients with unprotected left main disease, but PCI with DES is a reasonable alternative treatment option in those with favorable anatomy and high surgical risk.
Anticoagulation
Anticoagulant agents are an important adjunctive therapy for reperfusion therapy regardless of the strategy chosen (ie, whether it is primary PCI or fibrinolysis therapy). Different anticoagulation agents are available; the utility of each agent depends on the clinical context, taking into account the method of reperfusion.
For primary PCI, unfractionated heparin (UFH), bivalirudin, and low molecular weight heparin (LMWH) (eg, enoxaparin) are the available options. Fondaparinux is not used in this setting because of the increased risk of catheter thrombosis.
In patients receiving fibrinolytic therapy, anticoagulation should be given until revascularization is performed; if reperfusion is not feasible anticoagulants should be given for at least 48 hours or for the duration of hospital stay up to 8 days. UFH or LMWH may be used, with LMWH (enoxaparin) being preferred. Use caution with the administration of enoxaparin in patients older than 75 years as well as those with impaired renal function, because the use of enoxaparin is associated with a higher risk of intracranial bleeding. Bivalirudin may be used for patients who develop or have a history of heparin-induced thrombocytopenia (HIT) and require anticoagulation.
Antiplatelet agents
All patients with STEMI should receive an empiric loading dose of aspirin (150.5 to 325 mg) as early as possible and prior to reperfusion, regardless of the reperfusion method. A lifelong maintenance dose of (75 to 81 mg) daily should be prescribed to all patients after STEMI.
Other antiplatelet agents used for dual antiplatelet therapy are the P2Y12 receptor inhibitors (eg, clopidogrel, ticagrelor, prasugrel); a loading dose of these agents is given before or at the time of reperfusion and an extended duration maintenance dose is administered thereafter, depending on the method of reperfusion.
For patients undergoing primary PCI, a loading dose of 600 mg of clopidogrel, 180 mg of ticagrelor, or 60 mg of prasugrel should be given as early as possible or at the time of primary PCI. A maintenance dose of P2Y12 receptor inhibitors should be continued for at least 1 year for patients who receive a stent, either a BMS or a DES. A daily dose of 75 mg clopidogrel, 90 mg ticagrelor (twice daily), or 10 mg prasugrel is recommended. It is reasonable to discontinue P2Y12 receptor inhibitor agents prior to 1 year for patients who receive a BMS if there is evidence of increased bleeding.
Introducing ticagrelor after myocardial infarction in patients with previous ischemic stroke is associated with lower rates of recurrent ischemic stroke, without an increase in intracranial bleeding.
The use of prasugrel is not recommended for patients with a history of stroke or transient ischemic attack (TIA).
For patients who receive fibrinolytic therapy, a loading dose of clopidogrel 300 mg followed by a daily maintenance dose of 75 mg should be given, preferably for 1 year or a minimum of 14 days. The use of other P2Y12 receptor inhibitor agents in patients treated with fibrinolysis has not been prospectively studied.
Other antiplatelet agents that may be used in STEMI management are the intravenous (IV) glycoprotein (GP) IIb/IIIa receptor antagonists. The adjunctive use of GP IIb/IIIa agents at the time of PCI can be considered on an individual basis for a large thrombus burden or inadequate P2Y12 receptor antagonist loading. For patients receiving bivalirudin as the primary anticoagulant, routine adjunctive use of GP IIb/IIIa inhibitors is not recommended but may be considered in selected cases.
Non-ST-Elevation (NSTE) ACS
Key points in the management of patients with non–ST-elevation acute coronary syndrome (NSTE-ACS) (unstable angina and non-STE myocardial infarction [NSTEMI]) is early evaluation and assessment of hemodynamic and electrical stability, estimation of the overall risk in these patients, and guidance of therapy.
There are two alternative management strategies, either an early invasive strategy with angiography, with intent for revascularization with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG), or a conservative strategy with initial medical therapy and noninvasive cardiovascular imaging. Regardless of the strategy, both entail aggressive utility of medications such as anticoagulants, antiplatelet agents, beta blockers, statins, and possible use of angiotensin-converting enzyme (ACE) inhibitors for appropriate patient populations.
Patients with refractory angina, clinical evidence of heart failure, or hemodynamic or electrical instability who do not have serious comorbidities or contraindications to angiography/PCI should undergo an early invasive strategy.
An immediate early invasive strategy is also recommended for patient who are stable but at a high risk for clinical events. It is reasonable to consider an early invasive strategy within 24 hours of admission in patients with intermediate/high risk. For patients who fall outside this category, a delayed invasive strategy within 25 to 72 hours of admission versus a conservative (ischemia-guided) strategy may be considered.
Beta blockers
Beta blockers work by reduction of oxygen consumption of the myocardium by lowering the heart rate, blood pressure, and myocardial contractility. They also play an important role in reduction of reinfarction and complex ventricular arrhythmias.These agents are recommended to be given orally within the first 24 hours, preferably using one of the three drugs proven to reduce mortality in heart failure patients: metoprolol, carvedilol, or bisoprolol.
Beta blockers should not be given intravenously in patients with evidence of low cardiac output state (heart rate >110 beats/min or systolic blood pressure < 100 mmHg) and used with caution in elderly patients or in individuals with an unknown left ventricular ejection fraction. These agents should also not be given to patients who have a contraindication to beta blockers (eg, first-degree heart block with a PR interval >240 ms, second- or third-degree heart block without a cardiac pacemaker, recent cocaine use, severe/advanced active reactive airway disease).
In patients with chronic obstructive lung disease or chronic asthma, beta-1 selective beta blockers are preferred and should be initiated at low doses.
Calcium channel blockers
Non-dihydropyridine calcium channel blockers (eg, verapamil or diltiazem) should be given for recurrent myocardial ischemia only if there are contraindications to using beta blockers. Similar to beta blockers, use of non-dihydropyridine calcium channel blockers can also increase the likelihood of developing cardiogenic shock, thus, similar caution should be used when considering the use of these drugs.
Avoid short-acting nifedipine in patients who are not receiving beta blockers, as this may result in increased mortality in patients with ACS.
Antiplatelet agents
Aspirin
Nonenteric-coated chewable aspirin 150 to 325 mg should be given to all patients with NSTE-ACS as soon as possible after presentation.
A maintenance dose of aspirin 75-100 mg daily should be continued indefinitely.
Some clinical data suggest that maintenance dose of aspirin higher than 160 mg daily is associated with increased risk of bleeding with no clear improvement in outcomes.
P2Y12 receptor inhibitors
The use of P2Y12 receptor inhibitors in addition to aspirin has resulted in better outcomes, with a reduction of the incidence of cardiovascular death, MI, and stroke. The three P2Y12 receptor inhibitors most commonly used in the treatment of NSTE-ACS are described in this section, as follows:
- Clopidogrel
- Ticagrelor
- Prasugrel
All three agents are given with an initial loading dose, followed by a daily maintenance dose up to 12 months for all patients treated for NSTE ACS with either early invasive or conservative strategies.
With the wider use of new generation drug-eluting stents (DES), a shorter duration of P2Y12 receptor inhibitors of 3-6 months can be considered in patients who are at high bleeding risk.
Clopidogrel
A loading dose of clopidogrel 300-600 mg is recommended, followed by a maintenance dose of 75 mg daily.
Extrapolated results from the Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events (CAPRIE) trial demonstrated that clopidogrel can be used in patients with NSTE-ACS who are intolerant to aspirin.
Ticagrelor
Ticagrelor is a reversible inhibitor of the P2Y12 receptor that has a more rapid onset of action and a shorter half-life than clopidogrel; therefore, it is administered twice daily for maintenance. A loading dose of ticagrelor 180 mg is recommended, followed by a maintenance dose of 90 mg twice daily.
The Platelet Inhibition and Patient Outcomes (PLATO) trial compared clopidogrel to ticagrelor in patients with NSTE-ACS and concluded that patients receiving ticagrelor had lower events of MI, stroke, and overall mortality.
A unique side effect observed in patients taking ticagrelor is dyspnea, but this is rarely severe enough to cause termination of treatment.
Ticagrelor should not be used concomitantly with higher doses of aspirin (>100 mg daily).
Prasugrel
A loading dose of prasugrel 60 mg is recommended, followed by a maintenance dose of 10 mg daily.
Because of the unique metabolic conversion pathways of prasugrel, it has a more rapid and more consistent platelet inhibition than clopidogrel, which was demonstrated in the Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction (TRITON–TIMI) 38 trial. However, there was a concern of an increased bleeding risk in individuals treated with prasugrel.Therefore, major contraindication to the use of prasugrel are a previous history of stroke or transient ischemic attack (TIA), age over 75 years, and low body weight (< 60 kg).
Current clinical practice guidelines have different recommendations with regard to the use of prasugrel upfront in patients with NSTE-ACS. The American College of Cardiology/American Heart Association (ACC/AHA) guidelines do not recommend the use of prasugrel in this setting; however, its use can be considered for those undergoing PCI. The ESC guidelines, however, recommend the use of prasugrel upfront in patients treated for NSTE-ACS—provided there is no contraindication to its use.
Glycoprotein (GP) IIb/IIIa receptor inhibitors
The Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy (PURSUIT) trialand the Randomized Efficacy Study of Tirofiban for Outcomes and Restenosis (RESTORE) trialdemonstrated the efficacy of these agents in the treatment of NSTE-ACS.
The preferred GP IIb/IIIa receptor inhibitors are eptifibatide or tirofiban. Patients undergoing an early invasive strategy who received dual antiplatelet therapy with high-risk features are considered candidates to receive either of these two agents.
However, GP IIb/IIIa agents are associated with an increased risk of bleeding complications, and most of the clinical trials studying these drugs were completed prior to the release of the P2Y12 receptor inhibitors. Thus, their use in NSTE-ACS is limited currently.
Anticoagulant therapy
Anticoagulant agents are recommended to be given to all patients with NSTE-ACS, regardless of the initial treatment strategy, in addition to antiplatelet therapy. The following agents may be considered as treatment options from this group of medications.
Unfractionated heparin (UH)
An initial loading dose of 60 IU/kg (maximum 4,000 IU) with an initial infusion of 12 IU/kg per hour (maximum 1,000 IU/h) adjusted per activated partial thromboplastin time (PTT) is recommended to maintain therapeutic anticoagulation according to the specific hospital protocol. This regimen is continued for 48 hours or until PCI is performed.
A major disadvantage of the use of unfractionated heparin is the large interindividual variability and narrow therapeutic window.
Low molecular weight heparin (LMWH)
Enoxaparin is given at a dose of 1 mg/kg subcutaneously (SC) every 12 hours. It should be continued for the duration of hospitalization or until PCI is performed. A dose reduction is required for patients with impaired kidney function.
Enoxaparin results in a more predictable and efficient anticoagulation compared to unfractionated heparin, leading to reduction in recurrent MI events; however, there is possibly a higher bleeding risk in patients undergoing PCI.These findings were demonstrated in the Efficacy and Safety of Subcutaneous Enoxaparin in Non–Q wave Coronary Events (ESSENCE) trial.
Bivalirudin
Bivalirudin is direct thrombin inhibitor that is given as 0.1 mg/kg loading dose, followed by 0.25 mg/kg per hour only in patients managed with an early invasive strategy. This regimen is continued until diagnostic angiography or PCI.In the Acute Catheterization and Urgent Intervention Triage Strategy (ACUITY) Trial, the efficacy of bivalirudin was noninferior to the use of heparin plus GP IIb/IIIa.
Fondaparinux
Fondaparinux is a selective factor X inhibitor. This agent is given as a once-daily SC injection of 2.5 mg, which is continued for the duration of hospitalization or until PCI is performed.
Note that fondarparinux is contraindicated in patients with impaired kidney function. In addition, in patients undergoing PCI, administer another anticoagulant agent (eg, unfractionated heparin or bivalirudin), as fondaparinux is associated with a higher risk of catheter thrombosis; this was demonstrated in the Fifth Organization to Assess Strategies in Ischemic Syndromes (OASIS-5) trial.
Additional Aspects of Management and Late Hospital Care
After the initial management and stabilization of the patient in the early and critical phase of acute myocardial infarction (MI), the goals of care for these patients is to restore normal activities, prevent long-term complications, as well as aggressively modify lifestyle and risk factors. This multifaceted goal is achieved with the implementation of important key elements, including the use of cardioprotective medications and cardiac rehabilitation, as well as physical activity, diet, and patient education.
Cardioprotective medications
Inhibitors of the renin-angiotensin-aldosterone (RAA) system
Initiate angiotensin-converting enzyme (ACE) inhibitors and continue administration indefinitely in all patients with a left ventricular ejection fraction that is less than 40% and in those with hypertension, diabetes mellitus, or stable chronic kidney disease, unless contraindicated.
Angiotensin-receptor blockers (ARBs) are recommended in patients who are intolerant of ACE inhibitors.
Aldosterone blockers are recommended in addition to beta blockers and ACE inhibitors in patient who have had an MI with a reduced left ventricular ejection fraction of less than 40%, provided they have no renal impairment and have normal blood potassium levels (< 5 mEq/L). This was emphasized in the Eplerenone Post-acute myocardial infarction Heart failure Efficacy and Survival Study (EPHESUS).
Beta blockers
After an MI, all patients should be maintained on a beta blocker. Current clinical practice guidelines recommend use of one of three beta blocker agents proven to reduce mortality in patients with heart failure: metoprolol, carvedilol, or bisoprolol.
Statins
All patients with an acute MI should be started on high-potency statin therapy and continued indefinitely.
Current clinical practice guidelines, high potency statins such as atorvastatin 40 mg or 80 mg, or rosuvastatin 20 mg are recommended.
The Effects of Atorvastatin on Early Recurrent Ischemic Events in Acute Coronary Syndromes (MIRACL) trialand the Atorvastatin for Reduction of Myocardial Damage During Angioplasty-Acute Coronary Syndromes (ARMYDA-ACS) trialdemonstrated a reduction in mortality rates in patients who received high-potency statins after acute MI as compared to placebo.
Lifestyle modifications and cardiac rehabilitation
Much emphasis has been placed on post-discharge care for patients after MI.
Several lifestyle modifications have been strongly linked to a reduction in recurrent MI and prevention of further progression of cardiovascular disease. These modifications include dietary changes that adopt a low-fat and low-salt diet with dietary counseling, smoking cessation, up-to-date vaccination, and an increase in physical activity and exercise.
Referral to a well-structured cardiac rehabilitation program after MI should be considered for all patients, as this will promote patient compliance with the medical regimen and enhance lifestyle changes. In addition, aerobic exercise training within a cardiac rehabilitation program should be offered to patients after MI, with the need for an evaluation of both exercise capacity and exercise-associated risk.
The recommended frequency of regular exercise training is three or more times a week, for at least 30 minutes per session.
2019 ACC/AHA primary CVD prevention recommendations
The American College of Cardiology (ACC) and the American Heart Association (AHA) published recommendations on the primary prevention of cardiovascular disease (CVD) in March 2019.Ten key messages and a few recommendations from the guidelines are summarized below, including an emphasis on lifestyle choices/modifications and a major shift away from the broad use of aspirin in primary prevention.
◊ Key messages
A healthy lifestyle over a lifetime is the most important way to prevent atherosclerotic vascular disease, heart failure, and atrial fibrillation.
A team-based care approach is an effective strategy for CVD prevention. Clinicians should evaluate the social determinants of health that affect individuals to inform treatment decisions.
Adults aged 40-75 years being evaluated for CVD prevention should undergo10-year atherosclerotic CVD (ASCVD) risk estimation and have a clinician–patient risk discussion before being started on pharmacotherapy (eg, antihypertensive therapy, a statin, or aspirin). The presence or absence of additional risk factors and/or the use of coronary artery calcium (CAC) scanning can help guide decisions about preventive interventions in select individuals.
All adults should consume a healthy diet that emphasizes consumption of vegetables, fruits, nuts, whole grains, lean vegetable or animal protein, and fish, and minimizes the intake of trans fats, processed meats, refined carbohydrates, and sweetened beverages. In the setting of overweight and obesity, counseling and caloric restriction are recommended to achieve and maintain weight loss.
Adults, including those with type 2 diabetes mellitus (T2DM), should engage in at least 150 minutes per week of accumulated moderate-intensity physical activity or 75 minutes per week of vigorous-intensity physical activity.
For adults with T2DM, lifestyle changes (eg, improving dietary habits, achieving exercise recommendations) are crucial. If medication is indicated, metformin is first-line therapy, followed by consideration of a sodium-glucose cotransporter 2 inhibitor (SGLT2) or a glucagon-like peptide-1 receptor agonist (GLP-1).
At every healthcare visit, assess all adults for tobacco use. Assist tobacco users and strongly advise them to quit.
Aspirin should be used infrequently in the routine primary prevention of ASCVD because of a lack of net benefit.
Statin therapy is first-line treatment for the primary prevention of ASCVD in patients with elevated low-density lipoprotein cholesterol (LDL-C) levels (≥190 mg/dL), those with diabetes mellitus who are aged 40-75 years, and those determined to be at sufficient ASCVD risk after a clinician-patient risk discussion.
Nonpharmacologic interventions are recommended for all adults with elevated blood pressure or hypertension. When pharmacologic therapy is required, target the blood pressure to generally be below 130/80 mmHg.
Special considerations for elderly patients
Elderly patients should be treated aggressively. However, this patient population with MI is at an increased risk for developing complications, such as a greater risk of bleeding with thrombolytic therapy, but they also have the most to gain from this treatment.
Very elderly patient s should undergo primary angioplasty if available, but they should receive thrombolytic agents if excessive delay is anticipated before angioplasty can be performed.
Complications
Complications of myocardial infarction (MI) include arrhythmic complications, mechanical complications, left ventricular aneurysm formation, ventricular septal rupture, associated right ventricular infarction, ventricular pseudoaneurysm, and other issues.
Arrhythmic complications
Cardiac arrhythmias are not uncommon during and immediately after an acute MI. The incidence increases with ST-elevation MI STEMI and decreases with non-STEMI (NSTEMI). Of all patients who have an acute MI, about 90% develop some form of cardiac arrhythmias. In 25% of patients, such rhythm abnormalities occur within the first 24 hours. The risk of serious arrhythmias, such as ventricular fibrillation (VF), is greatest in the first hour and then declines thereafter.
Most peri-infarction arrhythmias are benign and self-limited. However, aggressively monitor and treat arrhythmias that result in hypotension, increase myocardial oxygen requirements, and/or predispose the patient to malignant ventricular arrhythmias.
Mechanical complications
The three major mechanical complications of MI, each of which can cause cardiogenic shock, are as follows:
- Ventricular free wall rupture
- Ventricular septal defect
- Papillary muscle rupture with severe mitral regurgitation
Left ventricular aneurysm formation
Left ventricular aneurysm is defined as a localized area of myocardium with abnormal outward bulging and deformation during systole and diastole. The rate of left ventricular aneurysm formation after acute MI is approximately 3-15%. Risk factors for these aneurysms after acute MI include the following:
- Female sex
- Total occlusion of the left anterior descending (LAD) coronary artery
- Single-vessel coronary artery disease (CAD)
- Absence of previous angina pectoris
Clinically, ventricular aneurysms may be recognized late, with symptoms and signs of heart failure, recurrent ventricular arrhythmias, or recurrent embolization.
Ventricular septal defect
Ventricular septal rupture (acute ventricular septal defect) is a rare but critical complication of MI. It occurs 2-8 days after an infarction and often precipitates cardiogenic shock. The differential diagnosis of postinfarction cardiogenic shock should exclude free ventricular wall rupture and rupture of the papillary muscles.
Ventricular rupture is more common in patients with anterior MI, individuals with hypertension, and those receiving nonsteroidal anti-inflammatory drugs (NSAIDs) or steroids.
To avoid the high morbidity and mortality associated with ventricular septal rupture, patients should undergo emergent surgery.
Concomitant coronary artery bypass grafting (CABG) may be required. Developments in myocardial protection and improved prosthetic materials have contributed greatly to successful management of ventricular septal rupture.Long-term survival can be achieved in patients who undergo prompt surgery.
Ventricular rupture occurs in the interventricular septum or the left ventricular free wall. Rupture in either location is a catastrophic event, with a greater than 90% mortality. Prompt recognition, stabilization, and surgical repair are crucial for patient survival. An echocardiogram can usually define the abnormality, and a right heart catheterization can show an oxygen saturation step-up in the case of a septal rupture.
Associated right ventricular infarction
Approximately one third of patients with inferior MI develop right ventricular infarction, which presents a special challenge because the adjunctive therapy, other than reperfusion, is somewhat different.
A right-sided electrocardiogram (ECG) with a more than 1-mm ST elevation in lead V3 R or V4 R describes a right ventricular infarction. An echocardiogram may be helpful in confirming the diagnosis.
On physical examination, signs of right-sided heart failure may be present, such as elevated jugular venous pulsation, right-sided S3, Kussmaul sign, or hypotension, but the patient may have clear lung fields.
The patient becomes volume dependent to maintain adequate left and right ventricular filling. Occasionally, dobutamine may be needed, or even an intraaortic balloon pump for hemodynamic support.
Avoid nitrates or any medications that lower preload in this setting. A pulmonary artery catheter can be helpful in guiding therapy.
Ventricular pseudoaneurysm
Complications of MI, such as ventricular pseudoaneurysms, are confirmed by means of echocardiography, magnetic resonance imaging (MRI), or contrast-enhanced computed tomography (CT) scanning. Imaging of a pseudoaneurysm typically shows a relatively narrow neck and a complete absence of muscle in the wall of the pseudoaneurysm—unlike a true aneurysm, which has a rim of myocardial wall that may be identified on angiography by the presence of mural vessels.
Miscellaneous complications
Left ventricular mural thrombus
Left ventricular mural thrombus is a well-known complication of acute anterior MI and frequently develops after left anterior wall infarction. The incidence of left ventricular mural thrombus as a complication of acute MI ranges from 20% to 40% but may reach 60% in patients with large, anterior-wall acute MIs who are not treated with anticoagulant therapy.
Left ventricular mural thrombus is associated with high risk of systemic embolization. Anticoagulant therapy may substantially decrease the rate of embolic events by 33% compared with no anticoagulation.
Pericarditis
The incidence of early pericarditis after MI is approximately 10%, and this complication usually develops within 24-96 hours after MI. Pericarditis is caused by inflammation of pericardial tissue overlying the infarcted myocardium. The clinical presentation may include severe chest pain, usually pleuritic, and pericardial friction rub.
Before the era of reperfusion, the incidence of post-MI pericarditis (Dressler syndrome) ranged from 1% to 5% after acute MI, but this rate has dramatically declined with the advent of thrombolysis and percutaneous coronary intervention (PCI).
Future and Emerging Therapies
Local injection of progenitor cells, growth factors, or stem cells may stimulate vascular development. Stem cell therapies for acute myocardial infarction (MI) remain a major target of research, with some data showing modest results.Investigators in the Reinfusion of Enriched Progenitor Cells And Infarct Remodeling in Acute Myocardial Infarction (REPAIR-AMI) study examined 204 patients with acute ST-elevation MI (STEMI) and reported greater improvement in left ventricular ejection fraction (LVEF) among patients who received intracoronary progenitor cell infusion than among those given placebo.
Several smaller clinical trials have suggested that intracoronary delivery of autologous bone marrow mononuclear cells (BMCs) have improved left ventricular function when administered within the first week following MI. However, results from the LateTIME Randomized Trial that evaluated whether intracoronary delivery of autologous BMCs delivered 2-3 weeks following first MI improved global and regional left ventricular function when compared with placebo suggested little improvement with this strategy in patients with MI and left ventricular dysfunction following reperfusion with percutaneous coronary intervention (PCI).
Medication Summary
The goals of pharmacotherapy for myocardial infarction are to reduce morbidity and to prevent complications. The main goals of emergency department medical therapy are rapid intravenous thrombolysis and/or rapid referral for percutaneous coronary intervention (PCI), optimization of oxygenation, reduction of cardiac workload, and pain control.
Antiplatelet Agents
Class Summary
Antiplatelet agents have a strong mortality benefit. There is an increased risk of bleeding in cases of emergency coronary artery bypass graft (CABG).
Aspirin (Ascriptin, Bayer Aspirin, Aspirtab, Ecotrin, Durlaza)
Early administration of aspirin in patients with acute myocardial infarction has been shown to reduce cardiac mortality rate by 23% in the first month.
Clopidogrel (Plavix)
Clopidogrel selectively inhibits adenosine diphosphate (ADP) binding to platelet receptors and subsequent ADP-mediated activation of glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation.
Clopidogrel may have a positive influence on several hemorrhagic parameters and may exert protection against atherosclerosis, not only through inhibition of platelet function but also through changes in the hemorrhagic profile.
This agent has been shown to decrease cardiovascular death, myocardial infarction, and stroke in patients with acute coronary syndrome (ie, unstable angina, non-ST elevation MI [NSTEMI], or ST-elevation MI [STEMI]).
Ticagrelor (Brilinta)
Ticagrelor and its major metabolite reversibly interact with the platelet P2Y12 ADP-receptor to prevent signal transduction and platelet activation. This agent is indicated to reduce the rate of thrombotic cardiovascular events in patients with acute coronary syndrome (ACS)—that is, unstable angina, non-ST elevation MI (NSTEMI), or ST-elevation MI (STEMI). Ticagrelor also reduces the rate of stent thrombosis in patients who have undergone stent placement for treatment of ACS, and it is indicated in patients with a history of MI more than 1 year previously. Patients can be transitioned from clopidogrel to ticagrelor without interruption of antiplatelet effect.
Prasugrel (Effient)
Prasugrel is a prodrug, a thienopyridine that inhibits platelet activation and aggregation through irreversible binding of active metabolite to adenosine phosphate (ADP) platelet receptors (specifically, P2Y12 receptor)
It is indicated for reduction of thrombotic cardiovascular events (including stent thrombosis) in patients with acute coronary syndrome (ACS) managed by means of percutaneous coronary intervention (PCI) who have either (a) unstable angina or non-ST-elevation MI (NSTEMI) or (b) ST-elevation MI (STEMI) when managed with primary or delayed PCI.
The use of prasugrel is not recommended for patients with a history of stroke or transient ischemic attack (TIA).
Vorapaxar (Zontivity)
Vorapaxar reversibly inhibits protease-activated receptor 1 (PAR-1) which is expressed on platelets, but its long half-life makes it effectively irreversible. It is indicated to reduce thrombotic cardiovascular events in patients with a history of MI or with peripheral arterial disease. It is not used as monotherapy but added to aspirin and/or clopidogrel.
Antithrombotic Agents
Class Summary
Antithrombotic agents, which include heparin, bivalirudin, and enoxaparin, prevent the formation of thrombi associated with myocardial infarction and inhibit platelet function by blocking cyclooxygenase and subsequent platelet aggregation. Antiplatelet therapy has been shown to reduce mortality rates by reducing the risk of fatal myocardial infarctions, fatal strokes, and vascular death. Unfractionated intravenous heparin and fractionated low-molecular-weight subcutaneous heparins are the 2 choices for initial anticoagulation therapy.
Bivalirudin (Angiomax)
Bivalirudin, a synthetic analogue of recombinant hirudin, inhibits thrombin; it is used for anticoagulation in patients with unstable angina who are undergoing PCI. With provisional use of glycoprotein IIb/IIIa inhibitor (GP IIb/IIIa inhibitor), bivalirudin is indicated for use as an anticoagulant in patients undergoing PCI. Potential advantages over conventional heparin therapy include more predictable and precise levels of anticoagulation, activity against clot-bound thrombin, absence of natural inhibitors (e.g., platelet factor 4, heparinase), and continued efficacy following clearance from plasma (because of binding to thrombin).
Heparin
Heparin augments the activity of antithrombin III and prevents the conversion of fibrinogen to fibrin. Heparin does not actively lyse, but it is able to inhibit further thrombus formation and prevents reaccumulation of a clot after spontaneous fibrinolysis.
Enoxaparin (Lovenox)
Enoxaparin enhances the inhibition of factor Xa and thrombin by increasing antithrombin III activity. In addition, it preferentially increases the inhibition of factor Xa. Enoxaparin is indicated for the treatment of acute STEMI managed medically or with subsequent PCI. It is also indicated for prophylaxis of ischemic complications caused by unstable angina and non-Q-wave myocardial infarction.
Dalteparin (Fragmin)
Enhances inhibition of factor Xa and thrombin by increasing antithrombin III activity. In addition, preferentially increases inhibition of factor Xa.
Except in overdoses, no utility exists in checking PT or aPTT, because aPTT does not correlate with anticoagulant effect of fractionated LMWH.
Average duration of treatment is 7-14 d.
Glycoprotein IIb/IIIa Inhibitors
Class Summary
Glycoprotein IIb/IIIa inhibitors prevent acute cardiac ischemic complications in unstable angina that is unresponsive to conventional therapy.
Abciximab (ReoPro)
Abciximab is a chimeric human-murine monoclonal antibody. It binds to the platelet surface glycoprotein IIb/IIIa (GPIIb/IIIa) receptor with high affinity, preventing the binding of fibrinogen and reducing platelet aggregation by 80%. Inhibition of platelet aggregation persists for as long as 48 hours after infusion stops.
Tirofiban (Aggrastat)
Tirofiban is a nonpeptide antagonist of the glycoprotein IIb/IIIa receptor. It is a reversible antagonist of fibrinogen binding, and when administered intravenously, it inhibits platelet aggregation by more than 90%.
Eptifibatide (Integrilin)
Eptifibatide is a cyclic peptide that also reversibly inhibits platelet aggregation by binding to the glycoprotein IIb/IIIa receptor. Blocks platelet aggregation and prevents thrombosis.
Vasodilators
Class Summary
Vasodilators relieve chest discomfort by improving myocardial oxygen supply, which in turn dilates epicardial and collateral vessels, improving blood supply to the ischemic myocardium.
Nitroglycerin IV (Nitro-Dur)
Nitroglycerin relaxes vascular smooth muscle via stimulation of intracellular cyclic guanosine monophosphate production, causing a decrease in blood pressure. Nitrates are useful for preload reduction and symptomatic relief but have no apparent impact on mortality rate in myocardial infarction.
Beta-adrenergic blockers
Class Summary
This category of drugs has the potential to suppress ventricular ectopy due to ischemia or excess catecholamines. In the setting of myocardial ischemia, beta-blockers have antiarrhythmic properties and reduce myocardial oxygen demand secondary to elevations in heart rate and inotropy.
Metoprolol (Lopressor)
This category of drugs, which includes metoprolol (Lopressor) and esmolol (Brevibloc), has the potential to suppress ventricular ectopy due to ischemia or excess catecholamines. In the setting of myocardial ischemia, beta-blockers have antiarrhythmic properties and reduce myocardial oxygen demand secondary to elevations in heart rate and inotropy.
Esmolol (Brevibloc)
Esmolol is a useful drug for patients at risk of experiencing complications from beta-blockers, particularly reactive airway disease, mild-to-moderate left ventricular dysfunction, and peripheral vascular disease. Its short half-life of 8 minutes allows for titration to desired effect, with the ability to stop quickly if necessary.
Atenolol (Tenormin)
Used to treat hypertension. Selectively blocks beta1-receptors with little or no effect on beta 2 types. Beta-adrenergic blocking agents affect blood pressure via multiple mechanisms. Actions include negative chronotropic effect that decreases heart rate at rest and after exercise, negative inotropic effect that decreases cardiac output, reduction of sympathetic outflow from the CNS, and suppression of renin release from the kidneys. Used to improve and preserve hemodynamic status by acting on myocardial contractility, reducing congestion, and decreasing myocardial energy expenditure.
Beta-adrenergic blockers reduce inotropic state of left ventricle, decrease diastolic dysfunction, and increase LV compliance, thereby reducing pressure gradient across LV outflow tract. Decreases myocardial oxygen consumption, thereby reducing myocardial ischemia potential. Decreases heart rate, thus reducing myocardial oxygen consumption and reducing myocardial ischemia potential.
During IV administration, carefully monitor blood pressure, heart rate, and ECG.
Angiotensin-Converting Enzyme Inhibitors
Class Summary
ACE inhibitors may prevent the conversion of angiotensin I to angiotensin II, a potent vasoconstrictor, resulting in lower aldosterone secretion. ACE inhibitors reduce mortality rates after myocardial infarction. Administer ACE inhibitors as soon as possible as long as the patient has no contraindications and remains in stable condition. ACE inhibitors have the greatest benefit in patients with ventricular dysfunction.
Captopril
Captopril has a short half-life, which makes it an important drug for initiation of ACE inhibitor therapy. It can be started at a low dose and titrated upward as needed and as the patient tolerates.
Enalapril (Vasotec, Epaned)
Enalapril prevents conversion of angiotensin I to angiotensin II, a potent vasoconstrictor, resulting in increased levels of plasma renin and a reduction in aldosterone secretion. This agent helps to control blood pressure and proteinuria.
Enalapril decreases pulmonary-to-systemic flow ratio in the catheterization laboratory and increases systemic blood flow in patients with relatively low pulmonary vascular resistance. It has a favorable clinical effect when administered over a long period. Enalapril helps to prevent potassium loss in the distal tubules. The body conserves potassium; thus, less oral potassium supplementation is needed.
Quinapril (Accupril)
Quinapril prevents conversion of angiotensin I to angiotensin II, resulting in increased levels of plasma renin and a reduction in aldosterone secretion.
Lisinopril (Zestril, Prinivil)
Prevents conversion of angiotensin I to angiotensin II, a potent vasoconstrictor, resulting in lower aldosterone secretion.
Angiotensin-Receptor Blockers
Class Summary
Angiotensin-receptor blockers may be used as an alternative to ACE inhibitors in patients who develop adverse effects, such as a persistent cough, although initial trials need to be confirmed. An angiotensin-receptor blocker should be administered to patients with STEMI who are intolerant of ACE inhibitors and who have either clinical or radiologic signs of heart failure or an LVEF of less than 40%.
Irbesartan (Avapro)
Blocks vasoconstrictor and aldosterone-secreting effects of angiotensin II at tissue receptor site. May induce more complete inhibition of renin-angiotensin system than ACE inhibitors and does not affect response to bradykinin (less likely to be associated with cough and angioedema).
Candesartan (Atacand)
Candesartan blocks vasoconstriction and aldosterone-secreting effects of angiotensin II. May induce more complete inhibition of renin-angiotensin system than ACE inhibitors, does not affect response to bradykinin, and is less likely to be associated with cough and angioedema. Use in patients unable to tolerate ACE inhibitors.
Valsartan (Diovan)
Produces direct antagonism of angiotensin II receptors. Displaces angiotensin II from AT1 receptor and may lower blood pressure by antagonizing AT1-induced vasoconstriction, aldosterone release, catecholamine release, arginine vasopressin release, water intake, and hypertrophic responses. Use in patients unable to tolerate ACE inhibitors.
Azilsartan (Edarbi)
Angiotensin II blocker; displaces angiotensin II from AT1 receptor and may lower blood pressure by antagonizing AT1-induced vasoconstriction, aldosterone release, catecholamine release, arginine vasopressin release, water absorption, and hypertrophic responses
May induce more complete inhibition of renin-angiotensin system compared with ACE inhibitors; does not affect response to bradykinin
Inhibits the pressor effects of an angiotensin II infusion in a dose-related manner
Eprosartan mesylate (Teveten)
Nonpeptide angiotensin II receptor antagonist that blocks vasoconstrictor and aldosterone-secreting effects of angiotensin II. May induce more complete inhibition of renin-angiotensin system than ACE inhibitors and does not affect response to bradykinin and is less likely to be associated with cough and angioedema.
For patients unable to tolerate ACE inhibitors.
Angiotensin II receptor blockers reduce blood pressure and proteinuria, protecting renal function, and delaying onset of end-stage renal disease.
Losartan (Cozaar)
Angiotensin II receptor antagonist that blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II. May induce a more complete inhibition of the renin-angiotensin system than ACE inhibitors, does not affect the response to bradykinin, and is less likely to be associated with cough and angioedema. For patients unable to tolerate ACE inhibitors.
Thrombolytics
Class Summary
The main objective of thrombolysis is to restore circulation through a previously occluded vessel by the rapid and complete removal of a pathologic intraluminal thrombus or embolus that has not been dissolved by the endogenous fibrinolytic system.
The first generation of fibrinolytic drugs (eg, streptokinase, urokinase, acetylated plasminogen streptokinase activator complexes [APSACs], reteplase, and novel plasminogen activator [nPA]) indiscriminately induced activation of circulating plasminogen and clot-associated plasminogen. First-generation drugs invariably elicited a systemic lytic state characterized by depletion of circulating fibrinogen, plasminogen, and hemostatic proteins and by marked elevation of concentrations of fibrinogen degradation products in plasma.
Second-generation drugs (eg, alteplase [t-PA], single-chain urokinase plasminogen activator), such as tenecteplase, preferentially activate plasminogen in the fibrin domain, rather than in the circulation, as with free plasminogen. Therefore, they have clot selectivity. Tenecteplase should be initiated as soon as possible in patients with STEMI; tenecteplase is administered as a single bolus, exhibiting a biphasic disposition from the plasma.
In optimal regimens, these agents induce clot lysis without inducing a systemic lytic state, they are less prone than nonselective agents to predispose the patient to hemorrhage necessitating transfusion, and they are effective in inducing recanalization in 80-90% of infarct-related arteries within 90 minutes. Therefore, t-PA recanalizes 75-80% of infarct-related arteries.
Alteplase, t-PA (Activase)
Alteplase (t-PA) is a fibrin-specific agent with a brief half-life of 5 minutes. Adjunctive therapy with IV heparin is necessary to maintain the patency of arteries recanalized by t-PA, especially during the first 24-48 hours.
Tenecteplase (TNKase)
Tenecteplase is a modified version of alteplase (t-PA) made by substituting 3 amino acids of alteplase. It can be given as a single bolus over a 5-second infusion, instead of 90 minutes with alteplase. Tenecteplase appears to cause less nonintracranial bleeding, but the risk of intracranial bleeding and stroke is similar to that of alteplase. Base the dose using patient weight. Initiate treatment as soon as possible after the onset of acute STEMI symptoms. Because tenecteplase contains no antibacterial preservatives, reconstitute immediately before use.
Analgesics
Class Summary
Pain control is essential to quality patient care. Analgesics ensure patient comfort, promote pulmonary toilet, and have sedating properties, which are beneficial for patients who experience pain.
Morphine sulfate (Duramorph, MS Contin, Kadian, Avinza)
Morphine sulfate is the drug of choice for narcotic analgesia due to its reliable and predictable effects, safety profile, and ease of reversibility with naloxone. Morphine sulfate is administered intravenously, may be dosed in a number of ways, and commonly is titrated until the desired effect is achieved.
PCSK9 Inhibitors
Class Summary
Over the last decade, inhibition of proprotein convertase subtilisin/kexin type 9 (PCSK9) has emerged as a promising target to reduce residual cardiovascular disease risk. PCSK9 is a protein that binds to low-density lipoprotein (LDL) receptors (LDLR) to promote their degradation. Monoclonal antibodies inhibit PCSK9 and thus prevent LDLR degradation. This action will increase the number of LDLRs and subsequently increase the clearance of LDL, ultimately lowering LDL-C levels.
In December 2017, the FDA approved the first PCSK9 inhibitor, evolocumab (Repatha), for the prevention of strokes, heart attacks, and coronary revascularizations.The approval was based on data from the evolocumab cardiovascular outcomes study (FOURIER). In the FOURIER clinical trial, evolocumab demonstrated significant benefits for 27,564 patients with established cardiovascular disease. The study revealed that when used in addition to optimized statin therapy, evolocumab reduced the risk of heart attack by 27%, the risk of stroke by 21%, and the risk of coronary revascularization by 22%. In addition, evolocumab showed a statistically significant 15% reduction in the risk of the primary composite endpoint, which included hospitalization for unstable angina, coronary revascularization, heart attack, stroke, or cardiovascular death.
In April 2019, the FDA expanded the indication for alirocumab (Praluent) to include risk reduction of MI, stroke, and unstable angina requiring hospitalization in adults with established cardiovascular disease.Approval was based on the ODYSSEY OUTCOMES trial (N=18,924) in patients with elevated LDL-C despite treatment with maximally tolerated statins. Patients who received injections of alirocumab 75 mg or 150 mg every other week achieved reduction in the risk for major cardiovascular events by 15% and all-cause death by 15% at a median follow-up of 2.8 years compared with those who received placebo.
Evolocumab (Repatha)
Human monoclonal IgG2 directed against PCSK9. Evolocumab binds to PCSK9 and inhibits circulating PCSK9 from binding to the LDLR, preventing PCSK9-mediated LDLR degradation and permitting LDLR to recycle back to the liver cell surface. By inhibiting the binding of PCSK9 to LDLR, evolocumab increases the number of LDLRs available to clear LDL from the blood, thereby lowering LDL-C levels.
Alirocumab (Praluent)
Monoclonal antibody that binds to PCSK9. LDL-C is cleared from the circulation preferentially through the LDL receptor (LDLR) pathway. PCSK9 is a serine protease that destroys LDLR in the liver, resulting in decreased LDL-C clearance and increased plasma LDL-C.

Leave a Reply
Want to join the discussion?Feel free to contribute!